|
USMS REVIEW, OF OIG DRAFT RECOMMENDATIONS
PRISONER MEDICAL CARE
I. USMS PROGRAM OVERVIEW
It is important that the background against which this program functions and the numerous factors which influence its effectiveness also be stated for the record. Every day, the 94 United States Marshals Service (USMS) district offices face an enormous level of workload and unlike other law enforcement agencies, field managers must respond effectively and promptly to a number of entities (i.e., federal judiciary, U.S. Attorneys, defense counsels, members of Congress, state and local governments, Bureau of Prisons (BOP), Department of Homeland Security, as well as prisoners and their relatives).
The USMS shares the Office of Inspector General s (OIG) concern for adequate prisoner security but increases in workload make this problematic. During FY 2003, the USMS received 154,400 individuals into custody, produced 587,700 for court, and transported an additional 411,800 by air and ground transportation modes. In coordination with the Office of the Federal Detention Trustee (OFDT), the agency is responsible for managing an annual detention budget of more than $800 million Each year new federal law enforcement initiatives are funded that generate an ever increasing workload for the agency however only a small percentage of the new positions included in the President's budget for the USMS have been funded by the Congress.
During the past 5 years the USMS average daily prisoner population grew by 53 percent (an increase of 15,300 new prisoners) Finding adequate detention space for such a large number of prisoners is a major challenge. Logistically, the district offices must locate detention bed space close enough to the 300 federal court cities to support the judicial process. Faced with such massive prisoner population increases, field staff have had to become increasingly dependent on guards to perform vital local transport functions.
The USMS also faces a national detention space crisis as it tries to find adequate bed space. There are only 3,618 jails in the United States Currently, 63 percent of USMS prisoners are housed in state and local facilities. It is compelling to note that only 2.8 percent of these facilities are certified by the American Correctional Association and 12.5 percent are certified by the National Commission on Correctional Health Care (NCCHC) The districts ability to track prisoner medical status is extremely limited as levels of medical care provided are determined by the attending physician of the jail. District staffs have no medical expertise. This situation is exacerbated by the lack of a centralized national prisoner database.
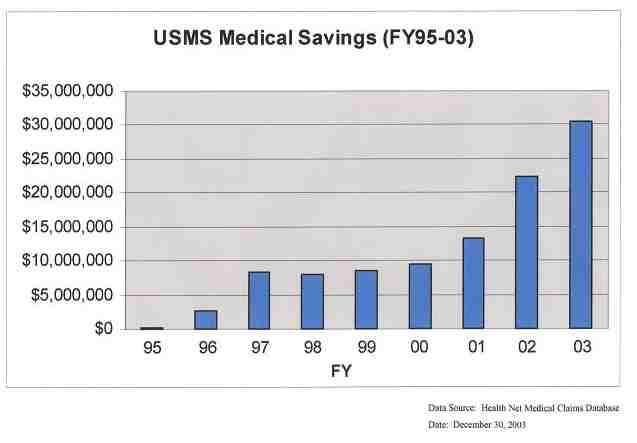
In spite of these program constraints, the USMS has done an outstanding job of developing and implementing an effective Prisoner Medical Program during the past 9 years. Not only has the agency developed and implemented extensive prisoner health care policies and procedures, it has managed to reduce prisoner medical costs by $103,126,945 (see attached). Such significant savings have been generated by the establishment of a national prisoner medical claims processing system and. the agency's success in obtaining passage of legislation for Medicare rates (Public Law 106-113) in November 1999. A major program success was achieved in 1999 when the USMS and Westchester County, New York, received the Department of Justice (DOJ), JustWorks Award for outstanding performance in developing a managed care network in the New York City area. This program success was made possible by taking an innovative interagency approach and obtaining vital technical support from the Department of Veterans Affairs (VA).
Throughout this process, the district offices have been directly involved in program development and steadfast in their support to implement procedural changes. While the USMS was able to partially implement the Medicare portion of this law through the use of a VA contractor, full compliance with this law is not possible until funding for a national managed care contract is provided. The USMS national managed care contract will also resolve a number of the OIG findings in this report.
It should be noted that the congressional conference language for the USMS, FY 04 appropriation, if enacted, will require the USMS to eliminate 85 administrative positions. This may adversely impact our ability to address the recommendations made in this audit report.
II. USMS COMMENTS ON OIG RECOMMENDATIONS
1. Ensure that districts adhere to established procedures for authorizing recording and tracking, outside medical procedures.
(a) Pre-Authorizations of Medical Procedures - The USMS will instruct district staff to improve their communications with jail medical staff on outside medical care referrals. It is the position of the agency that the successful implementation of a national managed care contract will resolve this problem. Under the terms of the scope of work of this contract, all outside medical care will be preauthorized by the USMS contractor in coordination with the district offices and the Office of interagency Medical Services (OIIvIS), Prisoner Services Division (PSD). The contract also requires creation of an interactive web site where districts will be 'required to concur, from a security aspect, on all preauthorized medical trips.
(b) Recording of Financial Transactions in the Financial Management System (EMS) - To the extent that this recommendation addresses the need for a consistent methodology for identifying, authorizing, recording and reporting medical expenses, the USMS concurs with the recommendation The Office of Finance, Management and Budget Division, will work with the district offices and OIMS to improve both the policies and procedures for recording and tracking these expenses.
To the extent that the recommendation refers to the different sub-object codes (SOC) used by district offices for recording guard costs associated with prisoner medical expenses, the USMS does not concur The difference between SOC 1150 and SOC 2555 is based upon the nature of the procurement. SOC 1150 is a personal service contract between the USMS and the guard performing the service. As such, this person is considered an employee of the USMS for income tax purposes and is reported under object class 1100 for external reporting to the Office of Management and Budget. Guards paid under 2555 are contract guards working for a vendor who has a contract with the USMS to provide such guard services. Payments to these vendors are, properly recorded under object class 2500. The nature of the underlying contractual relationship will dictate which sub-object class is charged.
(c) Prisoner Tracking System (PTS) - The USMS will instruct district staff to ensure that all required PTS entries are accomplished.
(d) Prisoner Case Files - The USMS will instruct district staff that prisoner case files (manual or paperless) must be properly maintained In particular, the field will be reminded that completed copies of Forms USM 552 (Prisoner Medical Records Release Form) and USM 553 (Medical Summary of Federal Prisoner/Alien in Transit) must be maintained for each prisoner.
(e) Federal Acquisition Regulations (FAR) - As already presented to the OIG Audit Team, the USMS will be able to efficiently resolve field FAR compliance issues with the award and implementation of a national managed care contract. It should also be noted that prior to the Office of General Counsel's (OGC) issuance of the December 3, 1999, memorandum on District FAR noncompliance issues, PSD had already worked with the Procurement Office to establish on December 1, 1998, a special Administrative Officers' Advisory Group for the Procurement of Health Care Services This group created a viable medical credit card program effective January 18, 2O01, which greatly enhanced field FAR compliance with medical service acquisitions This group also strongly recommended that a national managed care contract be established to resolve the remaining medical procurement issues.
Estimated Date for Completion of Actions - It is estimated that guidance for the field on audit compliance for items 1a-1d will be accomplished by February 27, 2004. Item 1e (FAR Compliance) will be subject to USMS receipt of the necessary resources to support this major initiative.
2. Re-initiate operational reviews of USMS district offices.
The USMS concurs with the OIG recommendation to re-initiate operational reviews of USMS district Offices The USMS is currently reviewing the position and staffing levels requited to establish an Office of Inspections that would include an expansion of the responsibilities of the current Program Review Office. The proposal currently under consideration would include an increased emphasis on the operational aspects of the work performed in the districts and the Office of Inspections would be under the management of a GS-1811 Criminal Investigator.
Estimated Date for Completion of Action - The USMS will keep the OIG advised of its progress in re-initiating these reviews.
3. Complete the on-going effort to negotiate a national managed health care contract for prisoner medical services that will remedy non-compliance with Title 18 U.S.C. 4006 and will effectively streamline the process.
The USMS fully anticipates awarding a national managed health care contract this fiscal year. Over the past few years, the agency did take steps in order to improve performance on the procurement of health care for prisoners until the national health care contract could be established. The USMS has implemented both a medical services credit card program and a national medical claims program. Both have afforded the agency to go from zero compliance to partial compliance on procurement regulations until the national managed health care contract is fully implemented this year.
On January 21, 2003, the Department of Health and Human Services' PCS issued a Request for Proposals (RFP) for the national managed health care contract. The Technical Evaluation Board (TEB) has begun meeting and soon will be entering the final stages of its evaluation process. If funding from this year's Federal Prisoner Detention Account is approved by the Office of the Federal Detention Trustee (OFDT) for this project, then an award can be made and national implementation will begin in late spring.
The USMS would like it noted that the original legislation proposed in September 1998 by the USMS, and formally supported by Justice Management Division, DOJ, did not have a provision that medical payments "shall not exceed the lesser of the amount under the...Medicare....Medjcaid program." Unfortunately, the legislative proposal was changed unexpectedly during the legislation process without input of the potential ramifications that such a change would have on the program office or the agency's resources needed to meet the new legislation.
The agency would also be concerned that the demand for only Medicaid rates may significantly result in the loss of a substantial number of medical care providers and a potential decline in the quality of medical care provided to prisoners. Physicians may refuse to treat USMS prisoners at Medicaid rates. In particular, medical specialists tend not to accept Medicaid rates for their specialized treatment. If this occurs, most specialty medical care would then have to be obtained by visits to the Emergency Rooms which presents a significant security concern. In fact, the USMS is so concerned about the adverse impact of the current legislation that on December 20, 2002 it submitted a formal legislative proposal to DOJ to modify this law and delete the Medicaid requirement. It is the agency's belief that it would be more appropriate to utilize private industry with a performance based procurement (as the USMS national managed care contract is currently structured) to obtain rates below the Medicare pricing structure.
The USMS is concerned with the accuracy of the audit report's claim that the agency expended $7 million more in medical finds than necessary. As confirmed in the exit interview, the amount was estimated using price averaging rather than a formal analysis of individual medical claims data.
Estimated Date for Completion of Action - Completion of this action will be subject to USMS receipt of the necessary resources to support this major initiative.
4. Enforce current USMS policy regarding the use of prisoners' private insurance to cover the costs of outside medical care.
The USMS will instruct district staff to ensure that the Form USM 552 (Prisoner Medical Records Release Form) is to be completed for all new prisoners at intake, a copy placed in the prisoner case file, and information on medical insurance is entered into PTS. It should be noted that in November 2001, OIMS conducted an informal survey of twelve districts (which represented approximately 42 percent of all USMS prisoners in custody) to determine the number of prisoners who might have medical insurance. The survey revealed that less than one percent (approximately 300 individuals of a population of 36,000 nationwide) might have such coverage. Even so, the position of the USMS is that any prisoner with medical insurance should be required to utilize that coverage as the financial benefits can be significant.
In an on-going high profile case in the Central District of California, OIMS and the district worked hard to enforce utilization of the prisoner's medical insurance to avert payment of approximately $1.2 million in medical care costs for the USMS. This is an excellent example of the benefits and mutual support of OIMS working closely with the field offices on medical case management.
Estimated Date for Completion of Action - It is estimated that guidance for the field on audit compliance will be accomplished by February 27, 2004.
5. Require that a management plan be created that ensures that deputy marshals are in compliance with cellblock health care policy and that they receive annual CPR and AED training in order to maintain certification.
(a) Prisoner Healthcare Policy Compliance - The USMS will require that district management conduct a formal review of all USMS prisoner health care policy with the appropriate district staff and provide to headquarters written certification of full compliance with cellblock policy and procedures.
Estimated Date for Completion of Action - It is estimated that guidance for the field on audit compliance will be accomplished by February 27, 2004, and district certification of policy compliance completed by April 30, 2004.
(b) CPR and AED) Training - The Judicial Security Division (JSD) will issue additional guidance to the field with regard to USMS policy on CPR and AED training.
Estimated Date for Completion of Action - It is estimated that a reminder for the field from JSD on USMS CPR and AED training requirements will be issued by February 27, 2004.
6. Strengthen the jail inspection program by:
(a) Ensuring the districts comply with USMS policy requiring an annual iail inspection. The PSD should maintain an IGA database which includes the date of the last inspection.
PSD has a database that records the current and future dates of all the jail inspections throughout the USMS. Currently, the USMS is working to update the system so reports can be generated to alert the districts that their jail inspections are due.
Estimated Date for Completion of Action - This database upgrade should be operational by the middle of 2004.
(b) Ensuring that district employees assigned as jail inspectors attend inspection training. including refresher courses, that contains a module on prisoner medical care. Employees conducting jail inspections should receive performance evaluations that include jail inspections as a rating element.
Jail Inspector training, otherwise known as Conditions of Confinement Training (CCT), has resumed as of June 2003. Two sessions have been conducted and three more are scheduled for 2004. A module on prisoner medical care is already included in the training. Refresher training will begin as soon as PSD is satisfied that all districts have an adequate number of trained jail inspectors. Then, past jail inspectors will begin to attend the new training. The latter two sessions in 2004, May and. August, will begin to include those inspectors who need refresher training.
With regard to changing rating elements for employees who hold the collateral assignment of jail inspector, these personnel are already evaluated on this duty as an element of their overall job performance. It is not necessary to separately evaluate the employee on a collateral duty.
Estimated Date for Completion of Action - Jail inspection training for all districts should be completed by the end of FY 2004.
(c) Requiring U.S. Marshals to review and improve their current jail inspection requirements. The reports for prisoner medical services should be more detailed and include supporting documents. The assessment tools provided in the CCRS should serve as a guide in improving the reports.
OFDT is currently working with BOP, USMS, and the Bureau of Immigration and Customs Enforcement (BICE) to improve the jail standards as well as the inspection process. PSD sees no need for more detailed medical service reports. Furthermore, the jail inspectors are not medical personnel and have limited medical knowledge. Any serious medical problems identified by district jail inspectors are to be referred to PSD for review.
Estimated Date for Completion of Action - Completion of this action will be determined by OFDT's completion of their interagency review of jail standards and the inspection process.
(d) Requiring districts to follow up on all CCR findings at least three years after the review has been completed. USMS inspection reports conducted on jail facilities that have submitted corrective action plans should include certification by the jail inspector that the jail is in compliance with the plan.
PSD is currently organizing a working group to review the CCR findings and coordinate action plans with district jail inspectors.
Estimated Date for Completion of Action - This project is planned for the summer of 2004.
7. Ensure that USMS Deputy Marshals Derform initial TB screening of the USMS prisoners that are housed in USMS district holding cells.
The USMS will require that district management conduct a formal review of all USMS prisoner health care policy with particular emphasis on airborne infectious disease control (TB) with the appropriate, district staff and provide USMS Headquarters with written certification of full district compliance with USMS cell block policy and procedures. However, it should be noted that district staff have no medical expertise and rely appropriately on the attending physician at the local detention facility to conduct intake medical screening, record medical histories, and determine appropriate medical care for each prisoner.
USMS cellblock personnel are directed by current USMS policy only to "visually screen for symptoms of TB" and isolate any suspected case of active infectious airborne disease (i.e., TB, SARS, etc.). OIMS has requested that JDIS or an upgraded PTS contain an expanded prisoner medical module that would permit national tracking of compliance and infectious TB cases by OIMS staff. This module would also have a cellblock intake screen which gives the intake cellblock deputy a "checklist" of medical items to review with the prisoner which can be immediately documented in the system. Such an approach is more efficient and effective than paper documentation.
Estimated Date for Completion of Action - It is estimated that guidance for the field on audit compliance and district certification of policy compliance will be accomplished by April 30, 2004. Modification of current or planned USMS automated systems will depend upon resource availability.
8. Ensure that all cases of active TB are reported directly to OIMS.
The USMS will require that district management conduct a formal review of all USMS prisoner health care policy with particular emphasis on airborne infectious disease control (i.e., TB, SARS, etc.) with the appropriate district staff and provide USMS Headquarters with written certification of full district compliance with TB control policy and procedures.
Estimated Date for Completion of Action - It is estimated that guidance for the field on audit compliance and district certification of policy compliance will be accomplished by April 30, 2004.
9. Require that prisoners' TB test dates and results be documented on the Form USM 553 Medical Summary of Federal Prisoner/Alien in Transit and entered into PTS. in accordance with USMS TB policy. Copies of the USM 553, either paper or electronic should be maintained at the district offices.
The USMS will instruct district staff to ensure that prisoner TB test dates and results are documented for each USMS prisoner on a Form USM 553 (Medical Summary of Federal Prisoner/Alien in Transit) by the appropriate local detention facility medical staff and those results are entered' into PTS and a completed copy of the form maintained in the prisoner case file.
Estimated Date for Completion of Action - It is estimated that guidance for the field on audit compliance will be accomplished by April 30, 2004.
10. Develop and implement a system to track and monitor active TB cases.
OIMS has continued to request that funding for an additional US Public Health Service Officer be provided so that an Infectious Disease Control Officer position could be created to track and monitor prisoner airborne infectious disease cases. Without adequate medical staff in OIMS and a national automated prisoner tracking capability, the agency will have to continue to rely on district communications to OIMS by phone and fax.
As stated previously, district staff have no medical expertise and rely on the attending physician of the detention facility to determine the health care needs of prisoners and to communicate those needs (if outside medical care is required) to the U.S. Marshal. Active TB is a reportable disease (under state and federal law) which means that local or state health departments must report all active cases to the Centers for Disease Control (CDC).
The USMS strongly agrees that field staff are responsible for ensuring that access to adequate health care (especially emergency care) is provided to all prisoners in USMS custody. Current USMS prisoner medical policy clearly directs field staff to obtain all emergency medical care immediately by contacting their local "911" service. District staff will also facilitate non-emergency care provided outside of detention facilities if such medical needs are known by the district, in accordance with USMS Prisoner Health Care Standards, and are verified by the attending physician. District staff should immediately confer with district management and OIMS medical staff when they are unsure on how to proceed. OIMS also maintains a United States Public Health Service (USPHS) Medical Duty Officer available 24 hours a day to assist district offices. These policies have been in effect since 1999.
In an effort to work and coordinate with other federal agencies as well as local jails in the DC area, USPHS nurses from OIMS participate in monthly meetings of the Washington Metropolitan Council of Government Subcommittee on Correctional Health Care (COG). This Subcommittee ensures informal and face-to-face liaison with regional community and federal detention facility health care managers that house USMS prisoners. The meeting format includes a medical case study presentation and discussion to identity and manage chronic and infectious disease seen in the correctional community, bench marking, communication and implementation of process to improve shared health care issues and concerns. Medical topics that have been discussed include HIV/AIDS, specifically bridging the gap between incarceration and release, Diabetes, Smallpox, Anthrax, SAPS, Palliative/End-Of-Life Care for pre- and post- release individuals, and newly approved pharmaceutical agents. This valuable forum provides a cross-sectional look into the challenges that are faced in the D.C. area (Virginia, Maryland, and the District of Columbia), keeps the OIMS staff members abreast of emerging health care issues in the detention community, and allows input and exchange from the USMS perspective on such issues as standards, formularies, transportation, costs and disease management as they relate to correctional health care.
It should also be noted that OIMS already receives approximately 2,000 medical cases for management and assistance from the field each year. As the USMS prisoner population continues to increase, medical case loads will grow dramatically as well as the pressure for receipt of additional OIMS medical resources.
Estimated Date for Completion of Action - Completion of this action will be subject to USMS receipt of the necessary resources to support this major initiative as well as completion of needed enhancements to existing USMS automated prisoner systems, The USMS remains firmly committed to ensuring that infectious airborne disease is adequately monitored and potential exposure to employees, other prisoners, and the public is prevented.
11. Develop and implement a policy for tracking and monitoring of HIV/AIDS and Hepatitis cases.
The USMS disagrees with this recommendation. The USMS relies on state and local jails, contract jails and BOP facilities to provide medical screening and medically necessary health services to USMS detainees. The USMS is not responsible for determining the medical status of its detainees, This responsibility falls on the attending physician at the facilities that house the detainees. The USMS is responsible for the costs of the medically necessary detainee health care that is ordered by the attending physician.
BOP has advised us that BOP correctional staff are not routinely provided information on the HIV status of inmates in BOP institutions. Such information is maintained in a separate inmate medical database, within the BOP's SENTRY system that is accessible only by BOP medical staff assigned to the BOP institution and BOP headquarters.
The National Commission on Correctional Healthcare (NCCHC) Standards for Health Services in jails recognizes that if a detainee is labeled HW positive, the detainee may be placed at undue risk for compromised personal safety. The standards provide that, in a detention setting, "it is particularly important that the rules of physician/patient confidentiality regarding HIV test results and diagnoses of AIDS be followed." See 2003 NCCHC Standards, Position Statement on Administrative Management of HIV in Corrections, p.189. Thus, the privacy of this information should be protected where possible.
Consistent with NCCHC standards, USMS detainee HIV and Hepatitis information is disseminated on a "need to know" basis and is not routinely shared with USMS staff. All USMS staff have been formally instructed to use universal precautions, in accordance with CDC guidelines and USMS policy, with regard to the searching, production, and transport of all detainees. In our view, it is inappropriate for USMS law enforcement staff to attempt to routinely diagnose, track, or document the HIV/Hepatitis status of USMS detainees except as otherwise required on a case-by-case basis.
Estimated Date for Completion of Action - No action is required.
12. Ensure that guard contracts are effectively monitored by:
(a) Requiring that the COTR submit comprehensive euard contractor evaluations every six months. These evaluations should be thorough and should require documentation that supports the determinations and findings of the COTR.
The USMS agrees that agency guard documentation management and training requirements for personal services guards need to be reviewed. As a result, PSD will establish a work group composed of members of field operations, field administration, PSD, and Procurement staff from the Business Services Division (BSD). The mission of this workgroup will be to review current USMS guard policy and procedures and oversee implementation of any modifications deemed necessary. In the interim, the USMS will require that district management conduct a formal review of the following priority program items and certify compliance:
(1) Ensure immediate and full compliance with the financial terms and all other conditions of all formal guard contracts currently in force.
(2) Comply with USMS training requirements for all guards.
Estimated Date for Completion of Action - The USMS guard work group should conclude their review and issue recommended corrective actions and policy changes by the end of the third quarter, FY 2004. Implementation will take place as soon as such policy changes have been approved and issued to the field and district management has had adequate time to implement needed changes.
With regard to the more immediate action items (guard contract terms and guard training), the USMS will require that district management conduct a formal review and provide USMS Headquarters with written certification of compliance by April 30, 2004.
(b) Requiring that the COTR submit to the contracting officer, along with the contractor evaluation, a list of the district's active contract guards. This list should include identifying information, prior experience, and training.
The USMS will instruct district management that formal evaluations and adequate documentation for formal guard company contracts must be maintained in accordance with current contract terms and conditions. Other OIG recommendations in this area will be considered by the USMS guard work group.
Estimated Date for Completion of Action - The USMS will require that district management conduct a review of all formal guard company contracts currently in force and provide written certification of compliance with contract terms and conditions by April 30, 2004.
(c) Requiring that the COTR evaluations elements be included in the personnel ratings, of USMS. employees assigned as COTRS.
All collateral duties are taken in to account when an evaluation is done on an employee.
Estimated Date for Completion of Action - No action is required.
|